If you’ve torn your ACL (anterior cruciate ligament), the standard story you’ll often hear is “you need surgery”. The actual clinical picture is more nuanced. Surgery is right for many ACL tears, but not for all of them, and the decision is more case-dependent than the default narrative suggests.
This article is an honest decision guide. What an ACL tear actually is, when surgery is genuinely the right call, when conservative care fits, and how to think about the choice.
For the broader knee picture, see our knee pain page.
Note on the slug spelling: “ligemant” is the misspelling on the originally indexed URL. The article body uses the correct spelling “ligament”.
What the ACL actually is
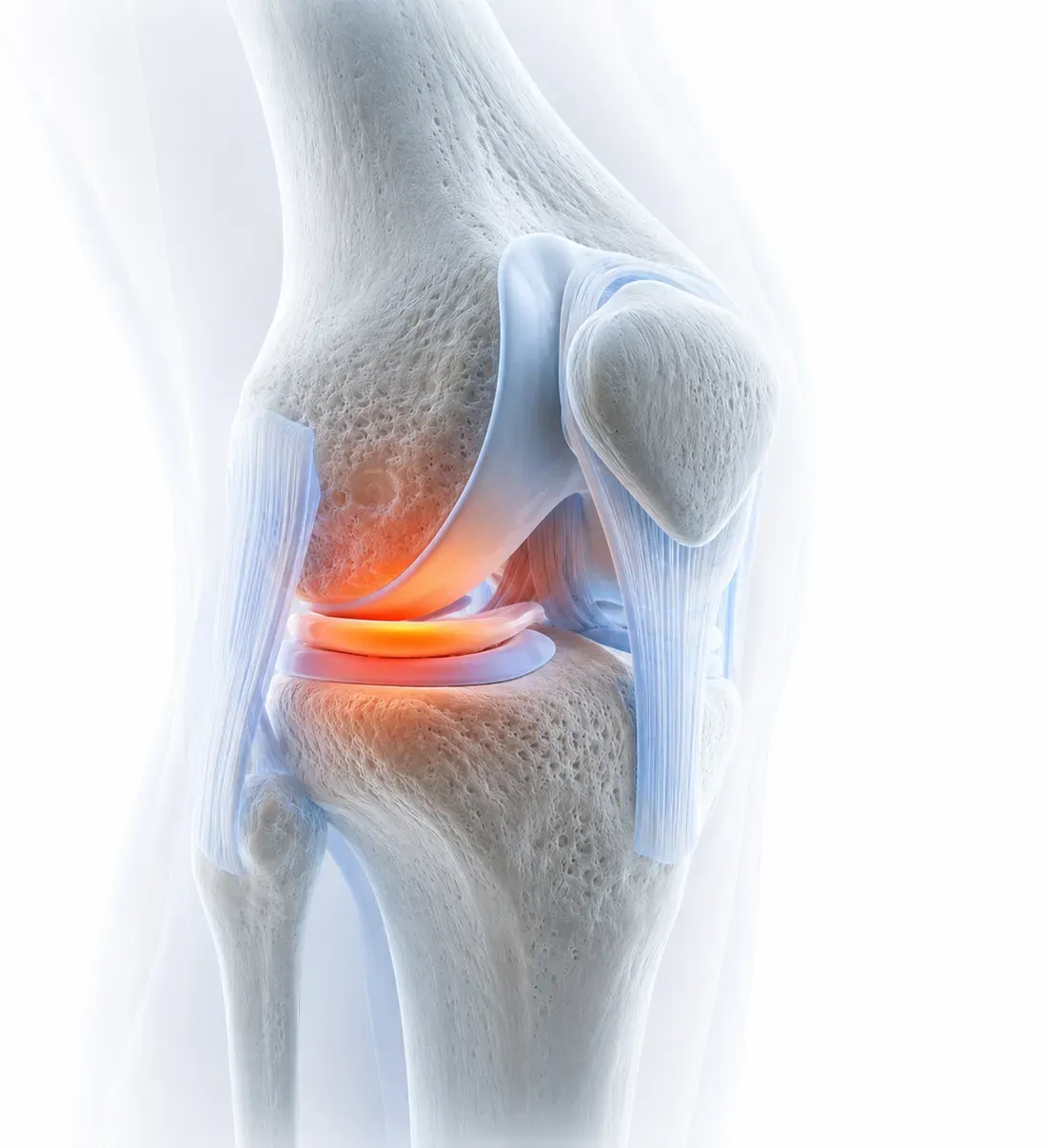
The ACL is one of four main ligaments stabilising the knee. It runs from the back of the femur (thigh bone) to the front of the tibia (shin bone), inside the joint. Its job:
- Prevents the tibia from sliding forward under the femur (the main mechanical role).
- Limits rotation between the femur and tibia.
- Provides position-sense feedback about where the knee is in space.
When the ACL tears, the knee loses some of that rotational and forward stability. Whether that loss matters functionally depends on what you’re asking your knee to do.
How ACL tears usually happen
The classic mechanism: a non-contact pivot. The foot is planted, the body twists, and the knee gives way. Common scenarios: skiing, netball, football, rugby, sudden direction changes in sport. The patient often hears or feels a “pop”, the knee swells significantly within hours, and walking becomes difficult.
Less common: direct contact (a tackle), a hyperextension event, a fall.
The diagnostic pathway
Clinical examination first. A skilled examiner can usually identify an ACL tear from the history and a few specific tests (Lachman, anterior drawer, pivot shift). An obvious “yes” or “no” can sometimes be made before imaging.
MRI confirms. ACL tears show clearly on MRI. The MRI also identifies common companion injuries (meniscal tears, articular cartilage injuries, other ligament involvement) which materially affect the decision.
Often there are companion injuries. ACL tears commonly come with damage to other structures. This is one of the variables in the surgical decision: an isolated ACL tear in an active patient is a different conversation from “ACL plus complex meniscal tear plus medial collateral injury”.
The surgical question, honestly
Standard advice (“you need ACL reconstruction”) is often appropriate, but isn’t universal. The surgical decision is genuinely a case-by-case judgement.
Surgery (ACL reconstruction) is more strongly indicated when:
- The patient is young and active (under 35-40), with sport or work that demands rotational knee stability.
- The patient experiences functional instability: the knee gives way during normal activity, not just sport.
- There are significant companion injuries (meniscal tears requiring repair, multi-ligament injury) where surgery is happening anyway.
- The patient has tried structured conservative care for 3-6 months and the knee remains unstable or unable to meet activity goals.
- The patient is a competitive athlete with specific competitive goals.
Conservative care is more strongly considered when:
- The patient is older or less active, with daily activities that don’t demand rotational stability.
- The patient is happy to modify activities (cycling, swimming, low-rotation gym work, walking) rather than return to high-pivot sport.
- There are no significant companion injuries.
- The knee is functionally stable in daily life after the acute swelling settles.
- Surgery carries specific risks for the patient (medical history, healing concerns, occupation factors).
The middle ground: many patients do well with 3 months of structured conservative rehabilitation as a trial, then reassess. If the knee is functionally stable and the patient’s goals are being met, conservative care can continue. If the knee remains unstable or the patient wants to return to pivot sport, surgical reconstruction is the right next step.
This pre-rehab approach is supported by good evidence (the KANON trial and follow-ups have shown comparable long-term outcomes for selected patients with delayed surgery vs immediate surgery), and it’s increasingly the default in NZ orthopaedic practice for non-elite-athlete cases.
What conservative care looks like
Whether as a definitive plan (chosen instead of surgery) or as a pre-surgical trial, conservative care follows a structured pathway:
Phase 1 (weeks 0-4): acute management. Pain and swelling control, restoring range of motion, gentle quadriceps and hamstring activation, normal walking pattern.
Phase 2 (weeks 4-12): rebuild quad and hamstring strength. Targeted strength work for both the surgical-side (where applicable) and the affected leg. Closed-chain exercises (leg press, squats to a comfortable depth). Single-leg work as tolerated.
Phase 3 (months 3-6): functional rebuild. Loading patterns specific to the patient’s goals. For active patients staying conservative, this includes graded return to running, cutting, and pivoting in a controlled way.
Throughout: education on what the knee can and can’t tolerate, when to push, when to back off, and how to recognise instability.
What pre-surgical rehab achieves
Even for patients heading for surgery, good rehab BEFORE the operation improves outcomes. The evidence is consistent: patients who go into ACL reconstruction with strong quads and full range of motion recover faster, regain strength sooner, and have better long-term function. Pre-surgical rehab usually runs 4-8 weeks (longer if needed).
The “do the surgery as fast as possible” instinct often costs more than it gains. Settle the swelling, regain range, build strength, then operate.
What recovery looks like (post-surgical)
The honest timelines:
- Walking unassisted: typically by 2-3 weeks.
- Driving (right knee or manual transmission): typically 4-6 weeks.
- Return to running: typically 3-4 months.
- Return to non-contact sport: typically 6-9 months.
- Return to contact / cutting sport: typically 9-12 months, sometimes longer.
- Full strength and confidence: 12-18 months.
These are typical for adult patients. Adolescent patients (whose growth plates are still open) and elite athletes have specific considerations.
The most common mistake: returning to pivot sport at 6 months because pain has settled, rather than at 9-12 months when strength and neuromuscular control are actually rebuilt. Re-injury rates are meaningfully higher for premature return.
Where Osteopathy fits
For ACL injuries, Osteopathy is one part of a multi-disciplinary picture, not the primary care.
What we contribute:
- Hands-on work for the surrounding knee, hip, and ankle structures that often get tight or under-activated during the recovery process.
- Assessment and treatment of compensatory patterns that develop in the unaffected leg or up the chain (back, hips, opposite knee).
- Coordination with surgical and physiotherapy teams for patients who want hands-on work alongside their main rehab pathway.
- Pre-surgical preparation for those heading toward operation.
- Long-term injury-prevention work for athletes returning to sport.
What we don’t do:
- ACL reconstruction surgery (orthopaedic surgeons).
- Primary post-surgical rehab in the public hospital pathway (typically physiotherapists are embedded in those teams).
- Imaging interpretation in isolation; we work from imaging done by GP, sports physician, or orthopaedic referral.
For most ACL cases in NZ, the pathway is: GP or A&E → orthopaedic referral → MRI → orthopaedic consult and surgical decision → physiotherapy-led rehab (with Osteopathy as a useful adjunct if patients want it).
ACC and ACL injuries
ACL tears are almost always ACC-eligible (a clear injury event with a clear mechanism). ACC funds the surgical pathway, the imaging, and the rehab. The patient’s role is mostly to lodge the claim at first contact and follow the pathway.
The ACC and Osteopathy guide covers the funded-care side, including how surgical referral and ongoing rehab work under ACC.
Booking with us
If you’re in the early days post-injury and want hands-on care alongside your medical pathway, book online or call us on 0800 67 77 00. We’ll work alongside your surgeon and physio (where applicable) and provide the targeted hands-on work that complements the rehab programme.
Related reading
- Knee pain condition page for the broader knee picture and our approach.
- How do injuries heal for the recovery framework.
- ACC and Osteopathy guide for the funded-care side.