Cycling puts the body in a sustained, slightly unnatural position for hours at a time. Over training cycles, miles, and seasons, that position can quietly produce predictable musculoskeletal patterns. The body adapts in ways that are functional for cycling but can become problematic off the bike (and sometimes on it).
This article is a practical guide for cyclists. The common patterns we see, the role of bike fit and training load, and how Osteopathy supports both injury management and ongoing performance.
The cycling position
Time in the saddle puts the body in a specific posture: hips flexed, knees moving in a narrow plane, spine forward-bent, neck extended to look forward, hands and arms taking weight, shoulders rolled forward. Hold any position for 4-8 hours a week and the body adapts to it.
The functional adaptations are useful for cycling but produce predictable secondary issues:
- Tight hip flexors from sustained hip flexion.
- Tight or weak glutes depending on riding style.
- Reduced thoracic spine extension from forward-bent posture.
- Tight pectorals and lats from the arm position.
- Tight neck extensors from looking up while spine is forward.
- Wrist and ulnar nerve issues from sustained pressure on the bars.
- Weak deep core function if not specifically trained.
None of this is unique to cycling; sustained postural patterns drive these in any activity. But cyclists tend to live in this pattern more consistently than most.
Common cycling-related issues we see
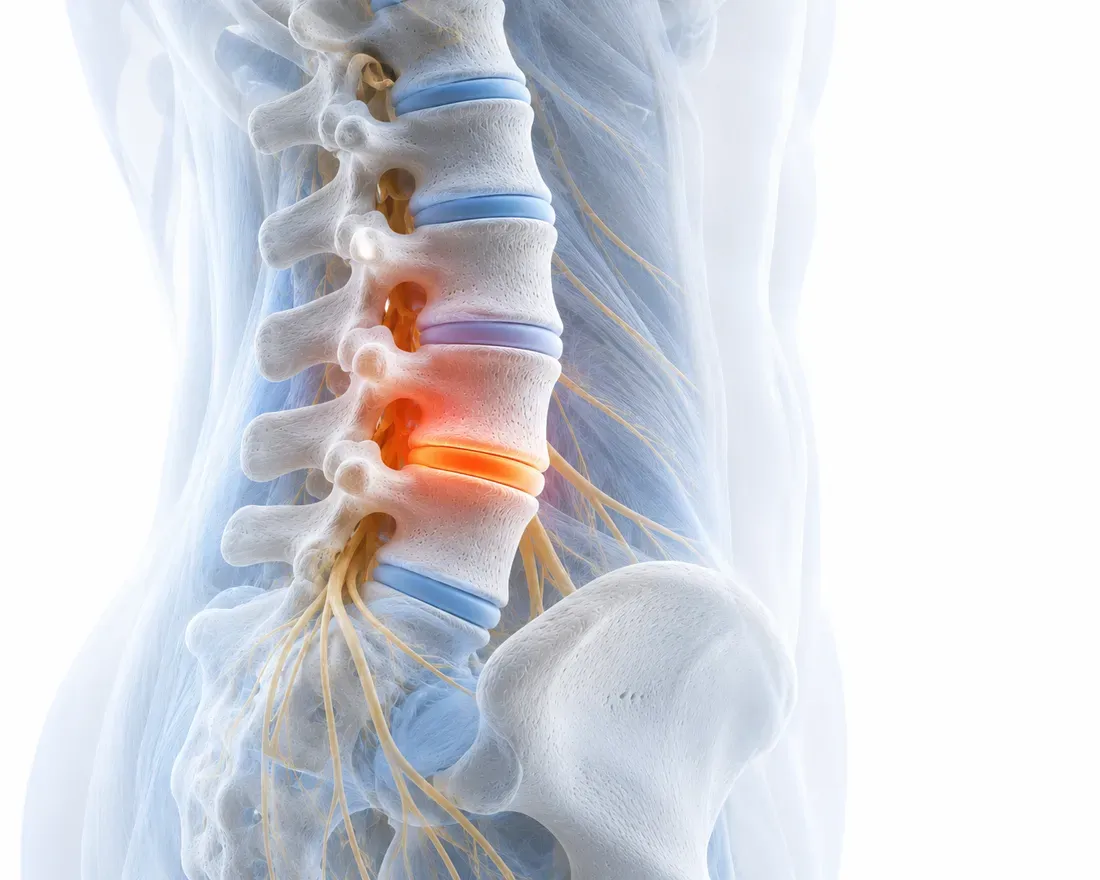
Low back pain. Most common. Sustained spinal flexion + hip flexion + weight on the saddle. Usually responds well to a combination of bike fit review, hands-on care, and specific strengthening.
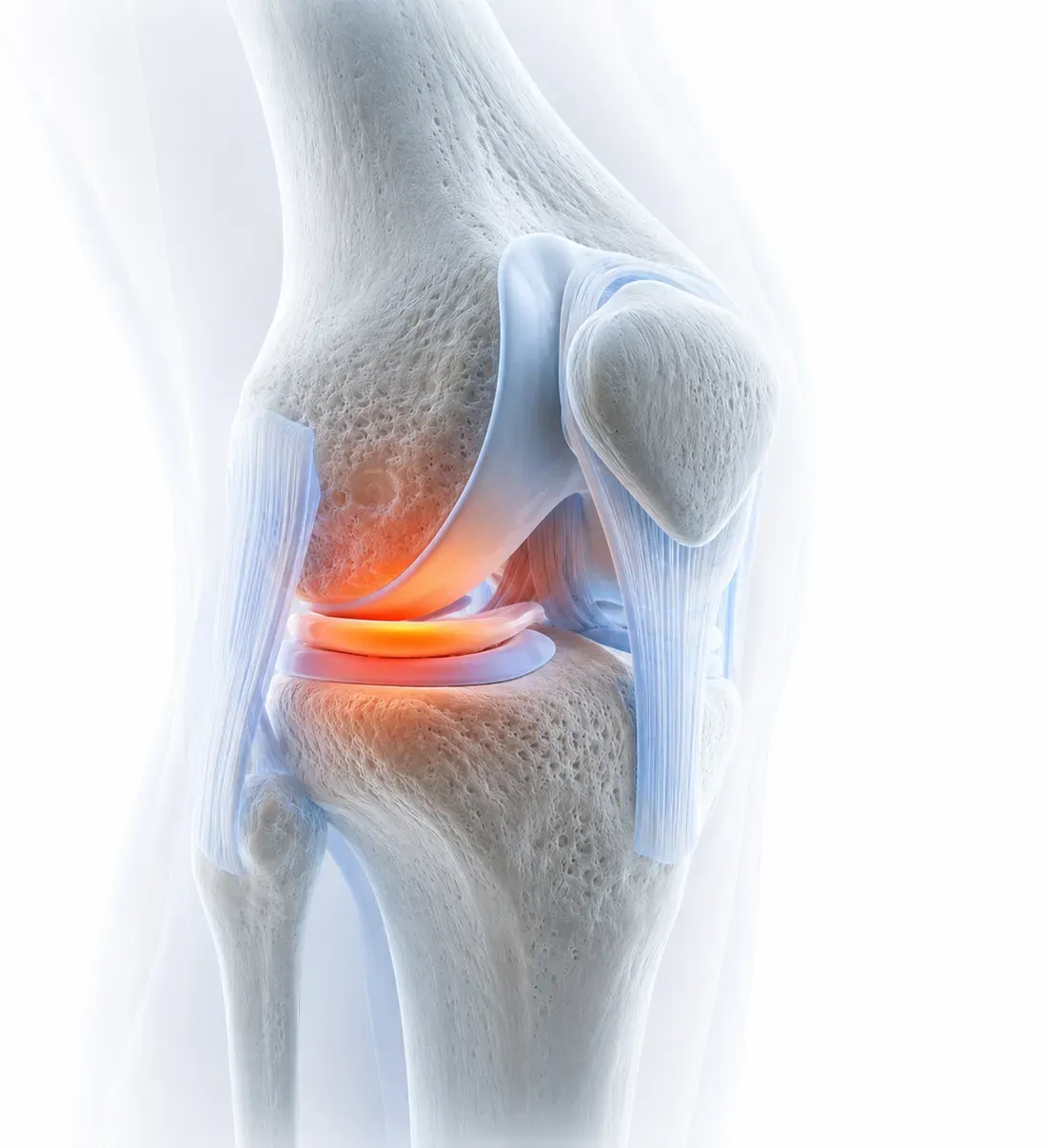
Knee pain. Often from saddle height/position, cleat alignment, or training load progression issues. Bike-fit review is critical here; sometimes a fix in 5 minutes saves months of treatment.
Neck and upper-back pain. From the head position, especially in aero/drop positions held for hours. Often combined with shoulder tightness.
Saddle / pelvic floor / perineal issues. A specialty area. Often involves saddle choice, position, and time. Sometimes warrants pelvic floor physiotherapy referral, especially for women cyclists with significant time in the saddle.
Wrist/hand numbness or pain (handlebar palsy). Pressure on the median or ulnar nerves where the wrist meets the bar. Bike fit + handlebar setup + grip variation often resolves it.
Calf or Achilles tightness. Often from cleat/pedal stroke patterns. Can affect off-bike walking and running tolerance.
ITB (iliotibial band) tightness. Common from saddle position issues + the repetitive plane of motion.
Where bike fit matters most
Bike fit is the foundation. A clinical assessment often picks up things a 30-second eye-test doesn’t, and the ROI is high:
- Saddle height: too low overloads knees; too high creates back and pelvis issues.
- Saddle fore-aft position: affects pedalling biomechanics and load distribution.
- Reach (handlebar position): affects neck, shoulder, and back load.
- Cleat position and alignment: affects knee tracking and force transfer.
- Bar width and angle: affects shoulder, neck, and hand comfort.
- Saddle choice itself: width, shape, padding. Highly individual.
Many cyclists ride bikes set up at the shop without a proper fit, then attribute issues to “getting older” or “training too hard”. Often the fix is millimetres of saddle adjustment or a different cleat position.
For serious cyclists, a professional bike fit (a session with a qualified bike fitter, sometimes integrated with a clinician) is one of the highest-leverage investments. For occasional or recreational riders, a clinical assessment that includes basic bike-fit principles is often sufficient.
Where training load matters
Cyclists often increase volume too fast. A jump from 4 hours/week to 8 hours/week in a couple of weeks puts new load on tissue that hasn’t adapted, predictably triggering issues. The general rule: build volume and intensity by ~10% per week, with rest weeks every 3-4 weeks.
Other training load issues we see:
- Insufficient off-bike strength work: the cycling-specific muscles get stronger but the supporting structures don’t, creating imbalances.
- Insufficient mobility work: tightness compounds across training cycles.
- Insufficient recovery between hard sessions: tissue doesn’t fully adapt before the next stress.
- Sleep and nutrition gaps: under-fuelled or under-slept training compounds slowly into issues.
Where Osteopathy specifically fits
For cyclists, Osteopathy contributes to:
Acute and overuse injuries. Standard hands-on care for the patterns above, with a cycling-aware framing.
Ongoing maintenance. Regular sessions (every 4-8 weeks for active cyclists) to address accumulated tightness and asymmetries before they become symptomatic.
Post-event or post-block recovery. After a major event or training block, restorative sessions to support recovery.
Bike-fit-aware assessment. Identifying when an issue is more likely a bike fit problem than a body problem (and referring to a bike fitter when appropriate).
Strength and mobility programming guidance. The off-bike work that supports on-bike performance and durability.
Coordination with sports medicine, physiotherapy, or coaching teams for cyclists with multi-disciplinary support.
A typical cycling-focused session
A first session for a cyclist usually includes:
- Detailed history: training volume and intensity, current goals, current bike setup, history of issues, off-bike activities.
- Examination: general musculoskeletal assessment + cycling-specific patterns (hip flexor tightness, thoracic mobility, glute activation, single-leg control, calf flexibility).
- Bike-fit assessment (where relevant; we don’t replace a professional bike fitter, but can identify obvious issues).
- Treatment: hands-on work targeting the specific patterns identified.
- Plan: ongoing session frequency, off-bike work, what to monitor, when to flag.
For ongoing-management cyclists, sessions every 4-8 weeks combined with consistent off-bike work usually keeps things stable.
ACC and cycling
Cycling injuries from a clear event (a crash, a fall, a road incident) are usually ACC-eligible. Gradual-onset overuse issues from training are often not. The ACC and Osteopathy guide covers the funded-care side.
Booking with us
If you’re a cyclist with a current issue or want a baseline assessment to inform your training and bike setup, book online or call us on 0800 67 77 00.
Related reading
- Care for sports athletes for the broader athletic-care page.
- How do injuries heal for the recovery framework.